
Overview
Chronic Obstructive Pulmonary Disease (COPD) – also known as Chronic Obstructive Lung Disease (COLD) – is a chronic inflammation of the lungs that causes obstruction of airflow1 and ineffective airway clearance. It is commonly caused by distinct disease processes such as Emphysema and Chronic Bronchitis. COPD is generally caused by long-term exposure to irritating gasses or particulate matter such as those produced by cigarette smoke1.
Asthma: Also known as Chronic Reactive Airway Disease is characterised by reversible inflammation and the reactive constriction of bronchial smooth muscle, hypersecretion of mucus and oedema. Although similar in presentation to COPD, Asthma is a response to an allergen and can be reversed in most cases.
Classification
There are two primary classifications of COPD; Emphysema and Chronic Bronchitis, often these types of COPD can appear concurrently in patients, although they are two distinct disease processes2.
Pathophysiology
 COPD is a progressive limitation of the airflow through the lungs, and is associated with abnormal breathing and inflammatory response of the lungs to noxious gasses or particles2.
COPD is a progressive limitation of the airflow through the lungs, and is associated with abnormal breathing and inflammatory response of the lungs to noxious gasses or particles2.
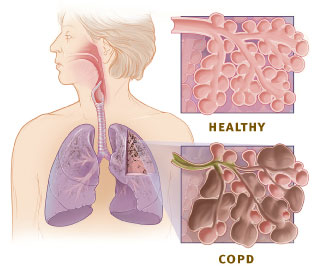
As causative gasses or particulates enter the lungs, they irritate the bronchioles or alveoli, leading to an inflammatory response in the proximal and peripheral airways. This inflammation causes narrowing of airways, creating a physical obstruction within the airways. This in turn, leads to an increase in the number of goblet cells, leading to hypersecretion of mucus which will manifest as a chronic productive cough.
As the condition progresses, scar tissue will form leading to further narrowing of the airway lumen, reducing elasticity of the airways. Alveolar wall destruction also occurs and leads to the loss of alveolar attachments and decreased elastic recoil2.
The chronic inflammatory process can also lead to changes in the pulmonary vasculature, causing a thickening of the vessel lining, increasing pre-load on the right atrium of the heart, and may lead to congestive heart failure.
Assessment
A diagnosis of COPD should be considered in any patients over the age of 40 who present with shortness of breath, history of a chronic cough, sputum production or frequent winter colds, combined with a history of exposure to risk factors3. SSpirometryis the preferred method of establishing lung function and confirming diagnosis. It is not recommended to screen patients who present asymptomatic or without risk factors4. A chest x-ray is also often taken to establish the severity of lung damage and establish a prognosis. Complete blood counts are also common to establish lung function, as well as exclude other conditions5.
Signs and Symptoms of COPD1
- Dyspnea
- Wheezing
- Barrel Chest.
- Weight loss.
- Excessive sputum production.
- Persistent cough or wheeze
- Chronic Cough.
Nursing Assessment
Prompt assessment of the respiratory system is essential in the nursing diagnosis.
During acute respiratory episodes in patients with COPD, it is important not to over oxygenate them. Aim for an SpO2 of 88-92%. More information about emergency oxygen for COPD Patients can be found here.
- Assess the patients risk factors.
- Assess the patients past and present medical History.
- Assess the signs and symptoms of COPD and establish their severity.
- Assess the patients vital signs.
- Assess breath sounds and pattern.
- Assess and monitor oxygen saturations.
Oxygen saturations lower than 92% on room air are not uncommon in COPD patients.
Management
Medical Management
Management of patients ith COPD takes a more reactive approach than a curative approach. Many cases of COPD are the result of prolonged smoking, and as a result, smoking cessation pathways are usually required.
Pharmacological interventions include both short-acting and long-acting bronchodilators to open airways. Inhaled corticosteroids are also often prescribed to reduce airway inflammation. Recently, severe COPD sufferers have been prescribed Phosphodiesterase-4 inhibitors, which acts to reduce airway inflammation and relax airways.
Acute infections like bronchitis and pneumonia are not uncommon in COPD patients, and so antibiotics are often used to treat acute exacerbations, however are not recommended for prophylactic treatment.
Surgical Management
 Surgical intervention is not indicated except in severe cases where a lung transplant may be necessary. The benefits of a lung transplant must be weighed against the life-long complications associated with transplantation. Transplantation also does not guarantee the condition will not recur, especially if the patient return to pre-diagnosis lifestyles, or where COPD is the result of heart failure.
Surgical intervention is not indicated except in severe cases where a lung transplant may be necessary. The benefits of a lung transplant must be weighed against the life-long complications associated with transplantation. Transplantation also does not guarantee the condition will not recur, especially if the patient return to pre-diagnosis lifestyles, or where COPD is the result of heart failure.
In severe cases, entire regions of the lungs may be destroyed, leading to the formation of a bullae (large air space within the lung) as seen in the scan on the right. In some cases, bullectomy may be indicated so improve airflow through the remaining lung.
Patient Education
Patients will need to be educated on how to self-manage their condition and identify when medical intervention may be required during acute exacerbations. Living with COPD can be a challenge as it will affect their ability to perform many basic activities. Climbing stairs or other physical activities can become unachievable, so patients will need to adjust their lifestyle to prevent exacerbating the condition.
Medication: Many patients will need to be educated on how and when to use their medications, the contraindications for any prescribed medications and any additional information relating to their medications.
Diet: A healthy diet will be beneficial to many COPD patients. Underweight patients may require nutritional supplements to increase strength and energy levels. Overweight patients can benefit greatly from adopting a healthy meal plan as weight loss can make breathing less labored, especially during physical exertionBROKEN! 3 .
Breathing Regulation: Patients should be educated on proper breathing techniques to minimise discomfort and maximise airway clearance. They should be instructed on proper positioning for breathing, as well as how to clear mucus from the airways. Drinking plenty of water can also help in clearing the airways of mucus.
Avoid Irritants: Smoking should be discontinued to prevent further damage and irritation to the airways and alveoli. Air pollution may also contribute to further lung damage. Patients should be advised to avoid places where other may smoke, as second-hand smoke may cause further irritation, and interfere with smoking cessation pathways.
Exercise: Regular exercise can seem difficult, but should exercise within tolerances can help to build strength and endurance, along with strengthening respiratory muscles.
Ongoing Monitoring: Patients will require regular check-ups with a GP or respiratory specialist. They should be encouraged to attend their doctor regularly, or if any changes occur in their condition.
Additional information in the form of a printout for patients can be found here.
Educational Video
Nursing Diagnosis & Care Plan
Nursing Priorities
Maintain airway patency and facilitate gas exchange. Enhance nutritional intake (additive for underweight patients, and subtractive for overweight patients). Educate patient on their condition, and how to self-manage the condition. Encourage the patient to exercise and build strength.
The ultimate priority is to prevent future complications and slow the progression of the disease.
Care Plan
Nursing Diagnosis: Ineffective airway clearance due to bronchoconstriction or hypersecretion of mucus.
Goal: Achievement of airway clearance and adequate oxygenation/ventilation to meet boy’s metabolic needs. Normal or normalised breath sounds.
Nursing Interventions:
- Appropriate administration of bronchodilators and corticosteroids.
- Perform actions to promote removal of secretions.
- Instruct and assist patient to breathe deep and cough every 1-2 hours.
- Maintain fluid intake to thin secretions and reduce drying of respiratory membrane.
- Humidify air as ordered.
- Perform suctioning if required.
- assist with, or perform postural drainage therapy if ordered.
- Discourage smoking.
- Decrease patient activity to prevent exacerbation of condition.
Consult appropriate health care professional (Doctor, respiratory therapist etc.) if signs or symptoms or increased impairment of gas exchange are present.
Nursing Diagnosis: Impaired gas exchange due to damage to alveolar sac resulting from chronic exposure to inhaled toxins
Goal: Improve ventilation and achieve sufficient oxygenation of body tissues.
Nursing Interventions:
- Auscultate breath sounds to establish areas of poor airflow.
- Encourage expectoration of sputum (suction may be required).
- Palpate for fremitus.
- Elevate head of bed to assist in breathing.
- Monitor vital signs with particular attention to SpO2 levels.
- Monitor level of consciousness.
- Administer oxygen as ordered, or if SpO2 level falls beyond acceptable range – notify treating physician.
Nursing Diagnosis: Ineffective breathing pattern6.
Goal: Patient will improve breathing pattern and maintain a respiratory rate within normal limits.
Nursing Interventions:
- Place patient in semi-fowlers position.
- Keep the patients back dry.
- change patient’s position every 2 hours if possible.
- Perform CPT to loosen secretions.
- Maintain patent airway and suction secretions as ordered.
- Provide oxygen as ordered to relieve dyspnea.
Nursing Diagnosis: Deficient knowledge.
Refer to patient education section under Management Tab.
Image credits: OpenStax JVP | Wikimedia
{kind=link}
Last revised: 5th June, 2017
[…] COPD […]